New
🛡️
Premium Quiz Locked
Nurse Mock Test Premium Premium unlock করতে payment করতে হবে।
📚 42 Quiz Setsকুইজ সেট
❓ 2100+ Questionsপ্রশ্ন রয়েছে
⏳ 15 Days Accessঅ্যাক্সেস সময়
₹30
🔐 এই premium quiz দেখতে হলে আগে register/login করুন।
👤 Register / Login করুন →
👤 Register / Login করুন →
কম্পিউটার📁 RAIL📁 WBCS📁 WBHRB স্টাফ নার্স📕 অর্থনীতি📕 ইতিহাস📕 ইংরেজি📕 কারেন্ট অ্যাফেয়ার্স📕 গণিত📕 জীবন বিজ্ঞান📕 জেনারেল ইন্টেলিজেন্স📕 প্রাক্টিস সেট (সমস্ত বিষয়)📕 ভূগোল📕 ভৌত বিজ্ঞান📕 মক টেস্ট📕 রাষ্ট্রবিজ্ঞান📕 সাধারণ জ্ঞান📗 RRB Group D📗 RRB NTPC📗 জুন কারেন্ট অ্যাফেয়ার্স📗 জুলাই কারেন্ট অ্যাফেয়ার্স📗মে কারেন্ট অ্যাফেয়ার্স
✅ Your Unlocked Premium Categories
আপনি যে premium categories কিনেছেন, সেগুলো নিচে দেখানো হলো। Category-তে click করলে সরাসরি quiz list/open হবে।
Loading...
🔒 Premium Access
Premium quiz কিনতে হলে আগে registration / login করতে হবে।
আগে register/login করুন, তারপর premium quiz কিনতে পারবেন।
Register করুন
Register করুন
আগে register/login করুন।
এই mobile number আগে ব্যবহার হয়েছে
নিচের user profile-এ এই mobile number দিয়ে আগে premium category/order করা হয়েছে। দয়া করে অন্য mobile number দিন।
Name-
Email-
Security reason-এর জন্য পুরো email দেখানো হচ্ছে না।
আপনি এই পৃষ্ঠার বিষয়বস্তু কপি করতে পারবেন না
📚
Subjects
👤
Quiz User
⏱
Remaining Time
--:--
0
Answered
0
Not
Answered
Answered
0
Not
Visited
Visited
0
Marked
for Review
for Review
0
Answered & Marked for Review
(will also be evaluated)
(will also be evaluated)
Quiz Panel
Choose a Question
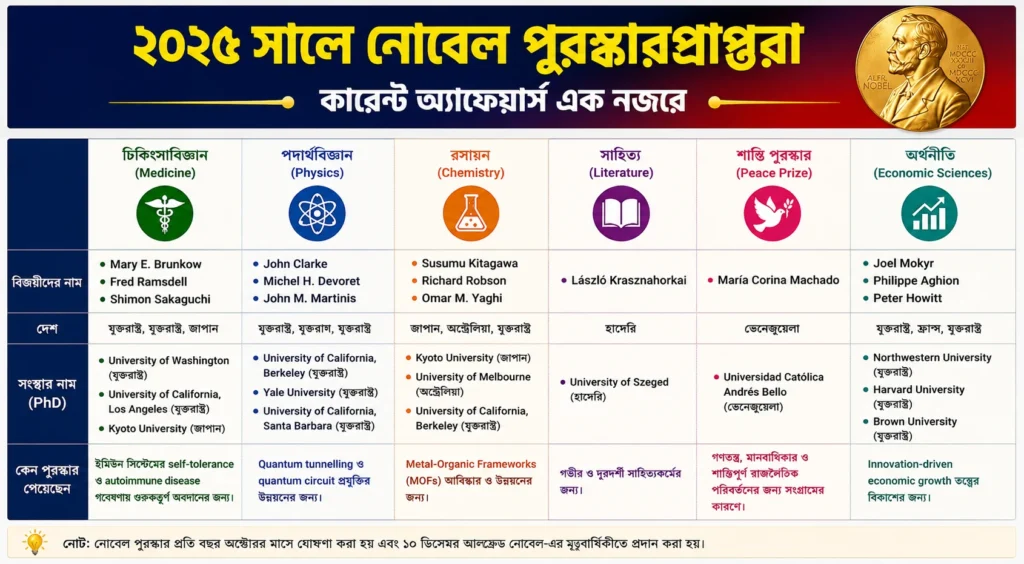
▣ Daily Current Affairs